
.svg)
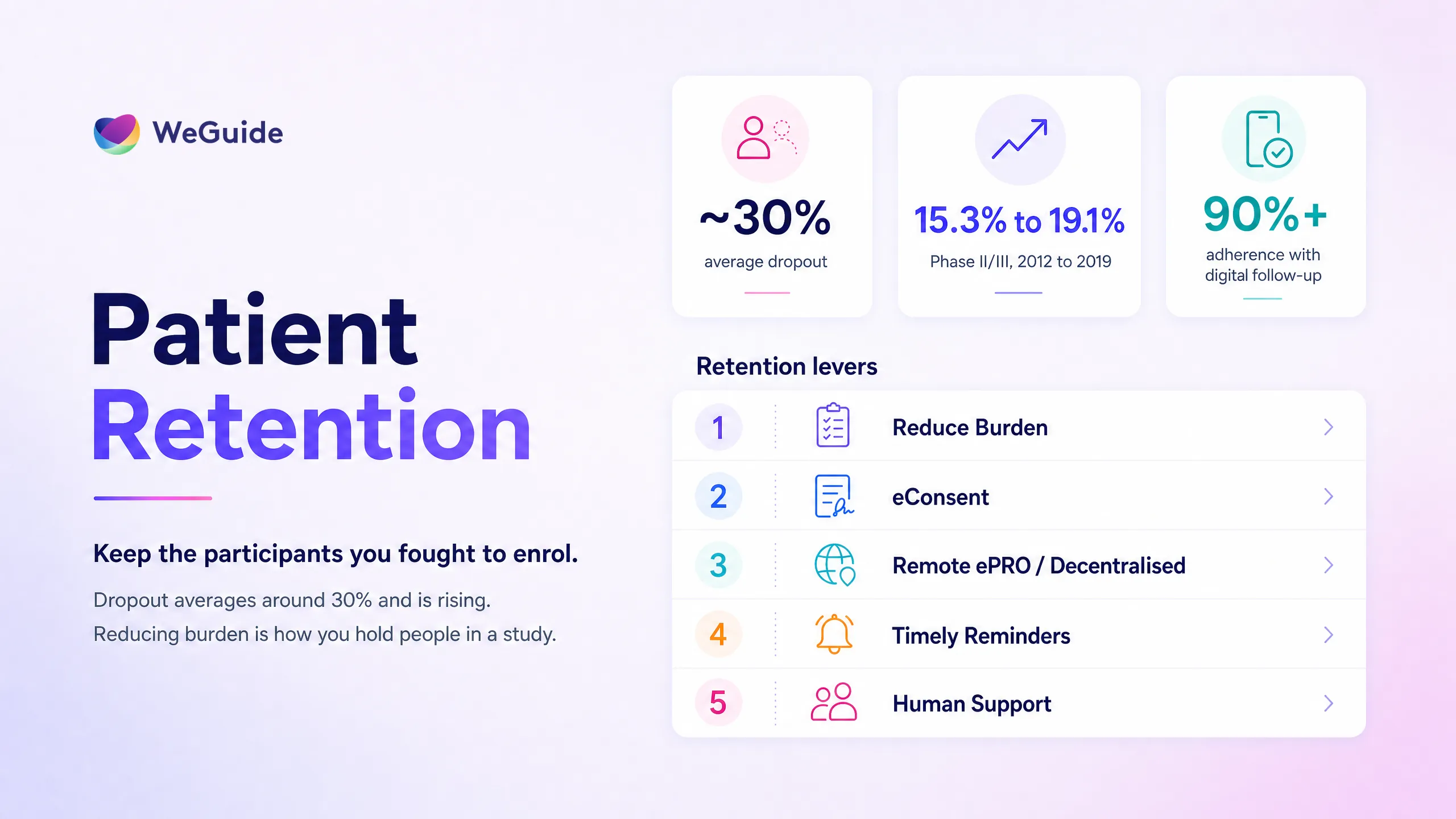

Patient retention in clinical trials is the share of enrolled participants who stay in a study until it finishes. Its opposite, called attrition, dropout, or withdrawal, averages roughly 30% across trials and has been climbing for years. Strong retention protects statistical power, data quality, timelines, and budget. The way to improve it is to cut participant burden and keep people engaged at every stage of the study.
Most teams pour their energy into recruitment, then watch participants they worked hard to enrol slip away between visits. That gap is expensive. A trial that enrols on time but loses a third of its participants can still miss its endpoints, blow its timeline, and weaken its results.
This guide covers what the usual advice leaves out. It gives you real dropout benchmarks, so you can tell whether your own numbers are normal. It maps the root causes of why participants leave. And it sets out a practical playbook of 12 ways to lift retention, ordered along the participant journey. We've spent more than 7 years building patient engagement software for studies like the BRACE Trial, so the playbook is grounded in what actually holds people in a study.
Key Takeaways
- Retention defined. Patient retention is the percentage of enrolled participants who complete a study. The inverse is attrition, dropout, or withdrawal.
- Dropout sits near 30% and the industry trend has worsened, rising from 15.3% in 2012 to 19.1% in 2019 across Phase II and III trials (Tufts CSDD).
- Burden is the throughline. Participant burden sits behind most dropout: too many visits, too much travel, and confusing or demanding tasks.
- Not all tactics work equally. A Cochrane review found reminders have little measurable effect, while modest monetary incentives have a moderate effect.
- Retention is designed in, not bolted on. The biggest gains come from reducing burden and supporting participants across the whole journey.
What Does Retention Mean in Clinical Trials?
Retention, often tracked as the completion rate, is the proportion of enrolled participants who stay in a study and complete the planned assessments. People use a cluster of related terms for the opposite, and they aren't quite interchangeable.
- Attrition is the overall loss of participants over the course of a study.
- Dropout and withdrawal describe a participant who actively leaves, whether they withdraw consent or a clinician removes them.
- Lost to follow up describes a participant who simply stops responding, without any formal withdrawal. Their data trails off, which leaves missing data and its own analysis headache.
The distinction matters because each one points to a different fix. A spike in withdrawals after a demanding visit signals a burden problem. A slow drift into lost to follow up signals weak engagement between visits. Tracking the reason, not just the count, is the first step to improving clinical trials patient retention.
Why Does Patient Retention Matter?
Retention matters because every participant you lose weakens the trial that's left. Dropout shrinks your effective sample, which erodes statistical power and can push a study below the threshold needed to detect a real effect. When the people who leave differ from the people who stay, you also get attrition bias, which skews the result itself.
The operational cost is just as real. Replacing a lost participant means more screening, more site time, and more delay. As a result, it's far more expensive than keeping the participant you already had. Industry surveys repeatedly find that a large share of trials struggle to retain enough participants to finish on plan. For sponsors and research teams, retention isn't a soft metric. It's the difference between a study that reads out cleanly and one that drags, costs more, and answers its question with less confidence.
If holding participants through to the end is the goal, clinical trial patient engagement software built for research is one of the most direct levers you have. We'll come back to how each capability maps to a specific cause of dropout.
What Is a Normal Clinical Trial Retention Rate?
Average dropout across clinical trials sits at roughly 30%, which puts typical retention near 70%. That headline hides a lot of variation. Dropout shifts with trial phase, therapeutic area, study length, and how heavy the protocol is. The clearest trend is that retention has become harder over time. Analysis from the Tufts Center for the Study of Drug Development found the industry dropout rate rose from 15.3% in 2012 to 19.1% in 2019 across Phase II and III trials, alongside growing protocol complexity.
Use the benchmarks below to sense check your own numbers rather than as fixed targets. Figures vary by protocol and population, so treat them as indicative.
| Segment | Typical dropout | Implied retention | Source |
|---|---|---|---|
| All trials (broad average) | around 30% | around 70% | Industry estimates |
| Phase II and III trend | 15.3% (2012) rising to 19.1% (2019) | around 81 to 85% | Tufts CSDD |
| Early oncology (Phase I) | under 10% | over 90% | Industry analysis |
| Women's health (Phase I) | around 16% | around 84% | Industry analysis |
| Palliative and advanced cancer | 26 to 44% | 56 to 74% | Published trials |
As a rough guide many teams use, losing more than 20% of participants starts to threaten the validity of a study. If your dropout is tracking above the benchmark for your phase and therapeutic area, treat it as an early warning rather than waiting for the final analysis to confirm the damage.
Why Do Participants Drop Out? Five Root Causes
Participants rarely leave for one tidy reason. A meta synthesis of withdrawal studies published in PMC grouped the reasons into a handful of recurring themes. Mapping your own dropout to these categories tells you which fix to reach for.
- How participants judge their own health. People who feel better, or who feel the study isn't helping, often disengage. Clear education about what the trial measures and why each visit counts helps here.
- Fit between the participant and the intervention. Side effects, a preference for a different treatment, or ending up in a control arm can all prompt withdrawal.
- Capability and comprehension barriers. When tasks are confusing, the app is clunky, or the consent never really landed, participation feels like work. This is where plain language and good design earn their keep.
- Concerns about the medication or procedures. Worry about safety or discomfort, especially around invasive assessments, drives people out.
- Life getting in the way. Travel, work, caring responsibilities, and the sheer time cost of visits push participants to quit, even when they support the research.
Underneath almost all of these sits one throughline: participant burden. The more a study asks of someone in time, travel, and effort, the more reasons they have to leave. Reduce the burden and most of these causes ease at the same time, and patient retention improves.
Built for the whole journey
Retention improves when you cut participant burden and keep people connected. See how WeGuide's participant-facing layer supports engagement at every stage.
Recruitment vs Retention, and Engagement vs Retention
These three terms get muddled, which leads teams to solve the wrong problem.
Recruitment is getting people enrolled. Retention is keeping them enrolled. A study can be brilliant at recruitment and still fail on retention, which is why a strong clinical trial recruitment strategy only gets you to the starting line. This article is about everything that happens after enrolment.
Engagement is the broader work of keeping participants informed, supported, and active. Retention is one of its main outcomes. Engaged participants are far more likely to stay, which is why the two are so closely linked. For the wider picture of how involvement and participant engagement fit together, see our guide to patient engagement in clinical trials.
12 Ways to Improve Patient Retention in Clinical Trials
Retention improves when you make participation easier and keep people connected to the study. The patient retention strategies in clinical trials below are ordered to follow the participant journey, from consent through to the final visit. Treat them as a menu, not a checklist, and be honest about which ones carry real evidence.
- Reduce visit and data entry burden. Every removable visit and every shortened form is a reason to stay. Audit the protocol for assessments that don't drive an endpoint, and move what you can to remote capture.
- Use plain language eConsent with comprehension checks. When participants genuinely understand what they signed up for, they stay longer. Interactive consent with short knowledge checks closes the gap that paper consent leaves open.
- Offer decentralised and hybrid options with remote ePRO and eCOA. Letting participants complete assessments from home through decentralised clinical trial tools removes the travel that drives so much dropout.
- Support participants in their own language. Multilingual access keeps diverse and CALD communities engaged instead of quietly dropping away when materials don't fit.
- Make scheduling flexible and reminders timely. Convenient visit windows and well timed prompts cut missed visits. A note of caution: a Cochrane review of retention strategies found reminders on their own have little measurable effect, so use them as a support, not a fix.
- Set expectations and keep educating. Participants who know what's coming, and why it matters, are less likely to be surprised into leaving. Deliver short education at the moments it's needed.
- Coordinate reimbursement and logistics. Smoothing travel, parking, and expense reimbursement removes a practical barrier. WeGuide helps coordinate and capture these workflows, but it doesn't disburse funds.
- Capture data passively with wearables. Devices like Garmin collect activity, heart rate, and sleep automatically, so participants contribute rich data without extra effort.
- Use telehealth for suitable visits. Video visits replace some site trips entirely, which is often the difference between a participant staying and quitting.
- Build a real relationship through personalised communication. Consistent, human, two way contact keeps participants feeling like partners rather than data points.
- Give data back to participants. Showing people their own progress and contribution respects their time and strengthens commitment.
- Monitor retention risk with analytics. Track completion and last activity in real time so you can spot at risk participants and reach out before they're gone, not after.
One honest note on incentives. The same Cochrane review that found reminders underwhelming found that modest monetary incentives have a moderate, measurable effect on retention. Many vendor guides treat every tactic as equally strong. The evidence doesn't, and planning around the difference is part of doing this well.
You can see this approach at scale in the BRACE Trial, run with the Murdoch Children's Research Institute. Across more than 6,000 participants in five countries, digital follow up and remote data capture sustained adherence above 90%, with no site visits needed for routine reporting. That's what engagement built into the design looks like in a real regulatory setting.
How to Build a Patient Retention Plan
A retention plan turns these tactics into something you can write into a protocol and operations document. Keep it stage based so each risk has an owner and a fix.
- At design. Map participant burden visit by visit, and cut or decentralise what you can before the protocol locks.
- At consent and onboarding. Use plain language consent, set clear expectations, and confirm comprehension.
- During active participation. Schedule flexibly, remind well, support reimbursement and travel, and keep education and communication flowing.
- Throughout. Watch retention metrics in real time with an analytics dashboard so at risk participants surface early enough to act on.
Written down and owned, a plan like this moves retention from a hope to a process. The upstream driver behind it is patient centricity in clinical trials, the operating model that puts participant needs at the heart of how a study is designed and run.
Frequently Asked Questions
Why is patient retention important in clinical trials?
Retention protects the trial's validity. Losing participants shrinks the sample, weakens statistical power, and introduces attrition bias when those who leave differ from those who stay. It also raises cost and delays timelines, since replacing a participant means more screening and site time.
What does retention mean in clinical trials?
Retention is the percentage of enrolled participants who remain in a study and complete its planned assessments. The opposite is attrition, made up of dropout and withdrawal, where participants actively leave, and lost to follow up, where participants stop responding without formally withdrawing.
What is the retention rate for clinical trials?
Retention varies by phase and therapeutic area, but a broad average is around 70%, meaning roughly 30% dropout. The trend has worsened over time, with industry dropout rising from 15.3% in 2012 to 19.1% in 2019 across Phase II and III trials, according to the Tufts Center for the Study of Drug Development.
What do you call it when a patient drops out of a clinical trial?
It's called attrition, dropout, or withdrawal when a participant leaves the study. When a participant simply stops responding without a formal withdrawal, it's called lost to follow up. Each term points to a different cause and a different fix.
How can decentralised trials improve retention?
Decentralised and hybrid designs let participants complete consent, surveys, and outcome assessments from home. By removing travel and site visits, they cut one of the biggest causes of dropout, which tends to lift retention, especially in longer studies and for participants who live far from a site. For a deeper look, see our guide to engagement and retention in decentralised trials.
How do you write a patient retention plan?
Build it around the participant journey. Map and reduce burden at design, use plain language consent at onboarding, support participants with flexible scheduling and reimbursement during the study, and monitor retention metrics in real time so you can reach at risk participants before they leave.
Holding Participants Through to the End
Patient retention in clinical trials comes down to a simple idea applied with care. Ask less of participants, support them better, and stay connected across every stage. The benchmarks tell you whether you have a problem, the root causes tell you where it sits, and the playbook gives you the moves to fix it.
Three things are worth remembering. Dropout averages around 30% and has been rising, so retention deserves planning, not afterthought. Participant burden is the cause behind most of it. And the tactics that work, from decentralised options to honest evidence based use of incentives, all share the same goal of making participation feel manageable.
Lift retention in your study
We can help you build the participant-facing layer that reduces burden and keeps people engaged from consent to final visit.
Book a demoNo pressure, just a conversation.

