
.svg)

Clinical trial patient engagement software is the participant facing layer of a study's technology stack. It's the app and tools that enrolled participants use to consent, report outcomes, learn about the protocol, and stay connected to the research team. Unlike a CTMS, which runs trial operations, or an EDC, which captures site data, this software exists to cut participant burden and protect retention.
If you're scoping one, the hard part isn't finding vendors. It's working out which capabilities you actually need, telling the category apart from the systems you already run, and justifying the choice internally. Most pages that rank for this term are either vendor product pitches or thin thought pieces, so they don't give you a way to compare tools.
This guide fixes that. You'll get a vendor neutral capability checklist you can lift into an evaluation document, a build versus buy framework, and an honest map of where one platform, patient engagement software from WeGuide, fits against it. We've spent more than 7 years building this layer for studies like the BRACE Trial, so the checklist reflects what actually holds participants in a study.
Key Takeaways
- It's the participant-facing layer — distinct from a CTMS (operations) and an EDC (site data capture).
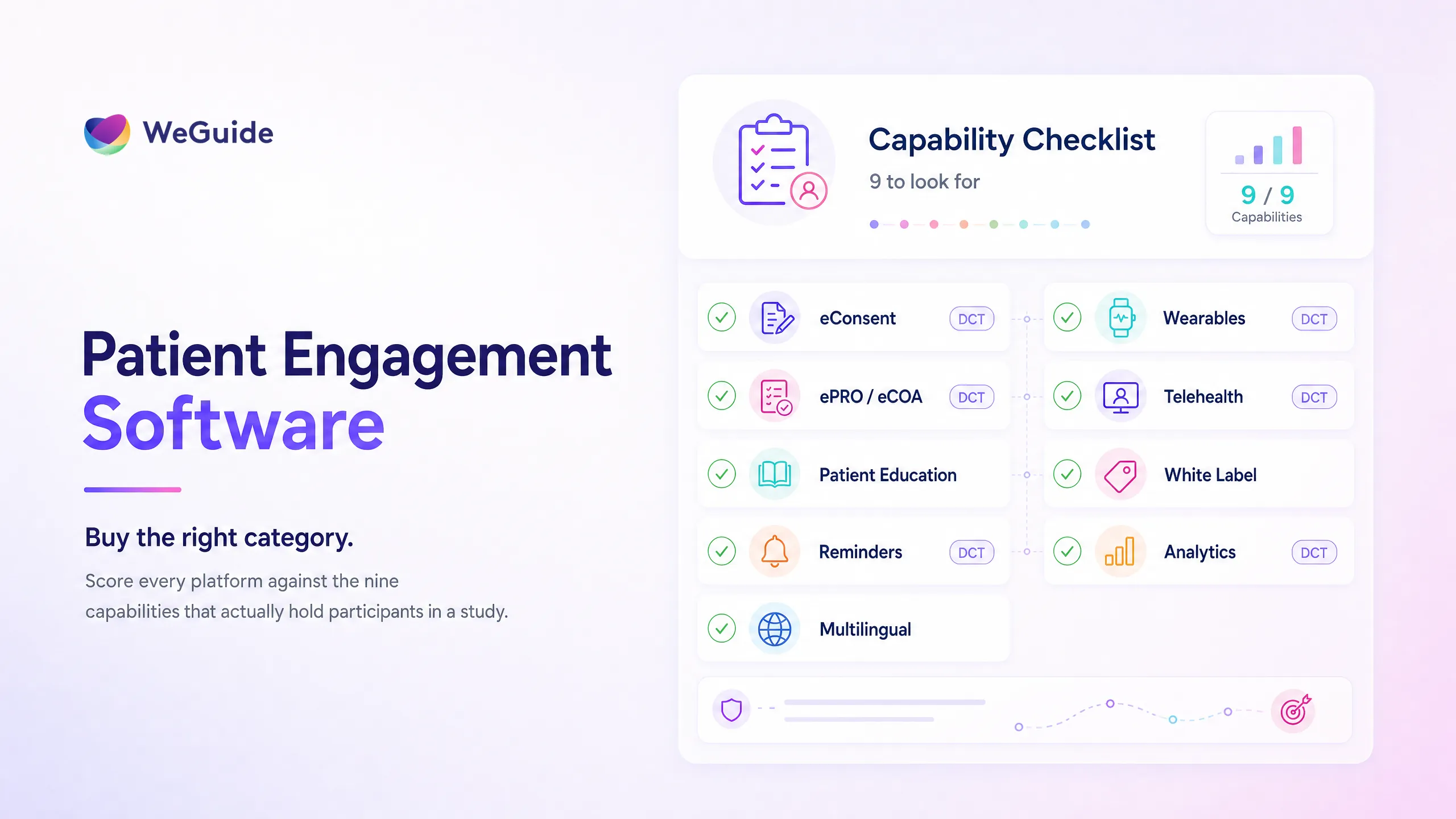
- Nine capabilities matter most: eConsent, ePRO and eCOA, patient education, reminders, multilingual access, wearables, telehealth, white-label branding, and analytics with integrations.
- Retention is the business case. Dropout averages around 30% and has been rising, and replacing a participant costs far more than keeping one.
- Buy rather than build in almost every case — pre-built compliance and faster validation usually beat a multi-year internal project.
- One participant app beats several point solutions, because separate ePRO and EDC systems create data-reconciliation work.
What Clinical Trial Patient Engagement Software Is, and What It Is Not
Clinical trial patient engagement software is the set of participant facing tools that keep enrolled people informed, supported, and active through a study. Participants use it to give consent, complete assessments, read protocol specific education, get reminders, and contribute data from their own device.
The fastest way to scope it is to separate it from the systems it sits beside.
- A CTMS runs the operations of a trial, including site management, scheduling, and finance. It's staff facing, not participant facing. Our guide to CTMS vs EDC covers the distinction in depth.
- An EDC captures and stores clinical data at the site. Engagement software often feeds participant reported data into it, but the two do different jobs.
- A recruitment CRO or platform finds and enrols participants. Engagement software takes over after enrolment, to keep those participants in the study.
So the category is narrow and specific. It's the participant layer, and its job is retention and data quality, not trial administration. This software is the tooling that delivers a broader operating model, so it helps to read it alongside our guide to patient centricity in clinical trials. For the wider picture, see our pillar on patient engagement in clinical trials.
Why It Matters: The Retention Math
The case for this software is retention. Dropout across clinical trials averages around 30%, and the trend has worsened, rising from 15.3% in 2012 to 19.1% in 2019 across Phase II and III trials, according to the Tufts Center for the Study of Drug Development.
That loss is expensive. By mdgroup's estimate, recruiting a participant costs around $6,500, while replacing one who drops out costs roughly $19,500, about three times more. Engagement tools attack the root cause, which is participant burden. Participants who use a well designed app to consent, report, and stay informed tend to be more adherent than those left with paper and clinic visits. The deeper case sits in our guide to patient retention in clinical trials.
Participants are receptive to this shift. In the CISCRP 2021 Perceptions and Insights study, 95% of participants said they would take part in a trial again, and most welcomed designs with fewer site visits. The question, then, isn't whether to give participants a better experience. It's what to look for when you buy the software that delivers it.
Attack the burden that drives dropout
WeGuide is the participant-facing layer built to protect retention, with eConsent, ePRO, education, and reminders in one branded app.
The Capability Checklist: 9 Things to Look For
This is the part to lift into your evaluation document. Score each platform against these nine capabilities, and treat the buyer question as the one to put to every vendor demo. WeGuide is mapped against the same list further down, honestly and in one place, rather than threaded through each point.
- eConsent. Remote and hybrid informed consent with multimedia explanation, comprehension checks, version control, and a full audit trail to 21 CFR Part 11. Ask: can participants consent and re consent remotely, and does every signature carry an audit trail?
- ePRO and eCOA. Electronic patient and clinician reported outcomes that participants complete on their own device, offline if needed, using validated instruments that flow into your EDC. Ask: does it support BYOD, offline capture, and clean export to our EDC?
- Patient education. In app, protocol specific education delivered at the right moment and in plain language, so participants understand what's asked and why. Ask: can we trigger education by study event, and translate it?
- Reminders and notifications. Push, SMS, and email prompts for visits and tasks, plus nudges when a participant looks at risk of dropping off. Ask: can reminders follow the protocol schedule and flag at risk participants?
- Multilingual access. Support for the languages participants actually speak, with a managed translation workflow rather than machine output, so CALD communities aren't excluded. Ask: which languages ship as standard, and how are translations managed?
- Wearables and device data. Passive capture from wearables and sensors, for example Garmin, so participants contribute objective data without extra effort. Ask: which devices integrate natively, and is the data clean enough for analysis?
- Telehealth and remote visits. Video visits that replace some site trips, which matters most in decentralised and hybrid designs. Ask: are remote visits part of the same participant app, or a separate tool?
- White label branding. A participant app under the sponsor's or site's brand, which builds trust and ownership of the participant relationship. Ask: can we ship a branded app to the App Store and Google Play?
- Analytics and integrations. Real time engagement dashboards plus an integration layer (API, FHIR, HL7) to connect with the EDC and CTMS. Ask: can we see engagement in real time, and does it connect to our existing stack?
| Capability | Why it matters | Buyer question | DCT critical? |
|---|---|---|---|
| eConsent | Compliant remote enrolment | Remote re consent with audit trail? | Yes |
| ePRO and eCOA | Clean participant data | BYOD, offline, EDC export? | Yes |
| Patient education | Comprehension and adherence | Event triggered and translated? | No |
| Reminders | Fewer missed visits | At risk flagging? | Yes |
| Multilingual | Inclusive recruitment | Managed translation? | No |
| Wearables | Objective passive data | Native device integration? | Yes |
| Telehealth | Replaces site visits | In the same app? | Yes |
| White label | Participant trust | Branded app to stores? | No |
| Analytics and integrations | Visibility and no data silos | Real time, API, FHIR? | Yes |
A note on breadth. Some platforms lead on one capability, such as a large pre validated instrument library, and you'll see vendors like Medable positioned that way. Use the checklist to weigh that against the capabilities your protocol actually needs, rather than buying the longest feature list.
Build or Buy
Almost every team should buy. Building your own participant app means specifying, developing, validating, and then maintaining it, while carrying the regulatory burden yourself. Reaching 21 CFR Part 11 and GDPR readiness on custom software takes months of documentation before your first participant enrols.
Buying gives you pre built compliance, faster validation, and a lower total cost of ownership, because hosting, security updates, and new features come with the licence. Building can make sense in rare cases, when you have a standing engineering team, a long horizon, and a need so specific that no platform fits. For most sponsors, sites, and CROs, that case doesn't hold.
One Platform or Several Point Solutions?
The other big choice is whether to run one participant app or stitch together several point solutions. Separate tools for consent, ePRO, and education each add a login for participants and a data stream for your team to reconcile.
When ePRO and EDC live in different systems, someone has to keep them aligned, and reconciliation is where errors and delays creep in. A single participant facing platform that exports cleanly to your EDC removes that overhead, and it gives participants one app instead of three. The fewer moving parts a participant sees across the clinical trial patient journey, the more likely they are to stay.
How WeGuide Maps to the Checklist
To be clear about positioning: WeGuide is the patient facing engagement and data capture layer for clinical trials. It's not a CTMS, not a traditional EDC, and not a recruitment CRO. It runs alongside those systems rather than replacing them.
Against the checklist, WeGuide covers eConsent with audit trails, ePRO and eCOA through the Form Builder, patient education, reminders, multilingual support, wearable capture through the Garmin integration, telehealth, white label apps, and real time analytics with an integration engine for EDC and EHR systems. On reimbursement, WeGuide helps coordinate and capture the workflow, but it doesn't disburse funds.
The proof that this layer protects retention is the BRACE Trial, run with the Murdoch Children's Research Institute. Across more than 6,000 participants in five countries, the study deployed in about six weeks and sustained adherence above 90% through remote symptom reporting, with no site visits for routine data capture.
Frequently Asked Questions
What is clinical trial patient engagement software?
It's the participant facing layer of a study's technology, the app and tools enrolled participants use to consent, report outcomes, learn about the protocol, and stay connected. Its purpose is to reduce participant burden and protect retention, which sets it apart from operational and data systems.
What features should clinical trial patient engagement software have?
Look for nine capabilities: eConsent, ePRO and eCOA, patient education, reminders, multilingual access, wearable integration, telehealth, white label branding, and analytics with integrations. Weight them against your protocol, and prioritise compliance, EDC integration, and at risk participant flagging for retention.
How is patient engagement software different from a CTMS or EDC?
A CTMS runs trial operations and an EDC captures site data, and both are staff facing. Clinical trial patient engagement software is participant facing. It supports consent, outcome reporting, and communication, and it usually feeds participant reported data into the EDC rather than replacing it.
Do patient engagement apps improve clinical trial retention?
Evidence suggests they help. Participants who use a well designed app to consent, report outcomes, and stay informed tend to be more adherent than those relying on paper and frequent site visits, because the app lowers the burden that drives most dropout. Retention still depends on study design, not the app alone.
Should we build or buy clinical trial patient engagement software?
Buy, in almost every case. A bought platform brings pre built 21 CFR Part 11 and GDPR readiness, faster validation, and lower total cost of ownership. Building only makes sense with a standing engineering team, a long horizon, and requirements no platform can meet.
Choosing With Confidence
Choosing clinical trial patient engagement software comes down to matching capabilities to your protocol and keeping the category clear in your head. It's the participant layer, separate from your CTMS and EDC, and its job is retention.
Score platforms against the nine capabilities, favour buying over building, and prefer one participant app over several point solutions you'll have to reconcile. Do that, and you'll buy the right category the first time and have the evidence to justify it.
See the checklist run against your study
We'll walk through all nine capabilities with a single participant-facing platform, and show where it fits beside your CTMS and EDC.
Book a demoNo pressure, just a conversation.

