
.svg)
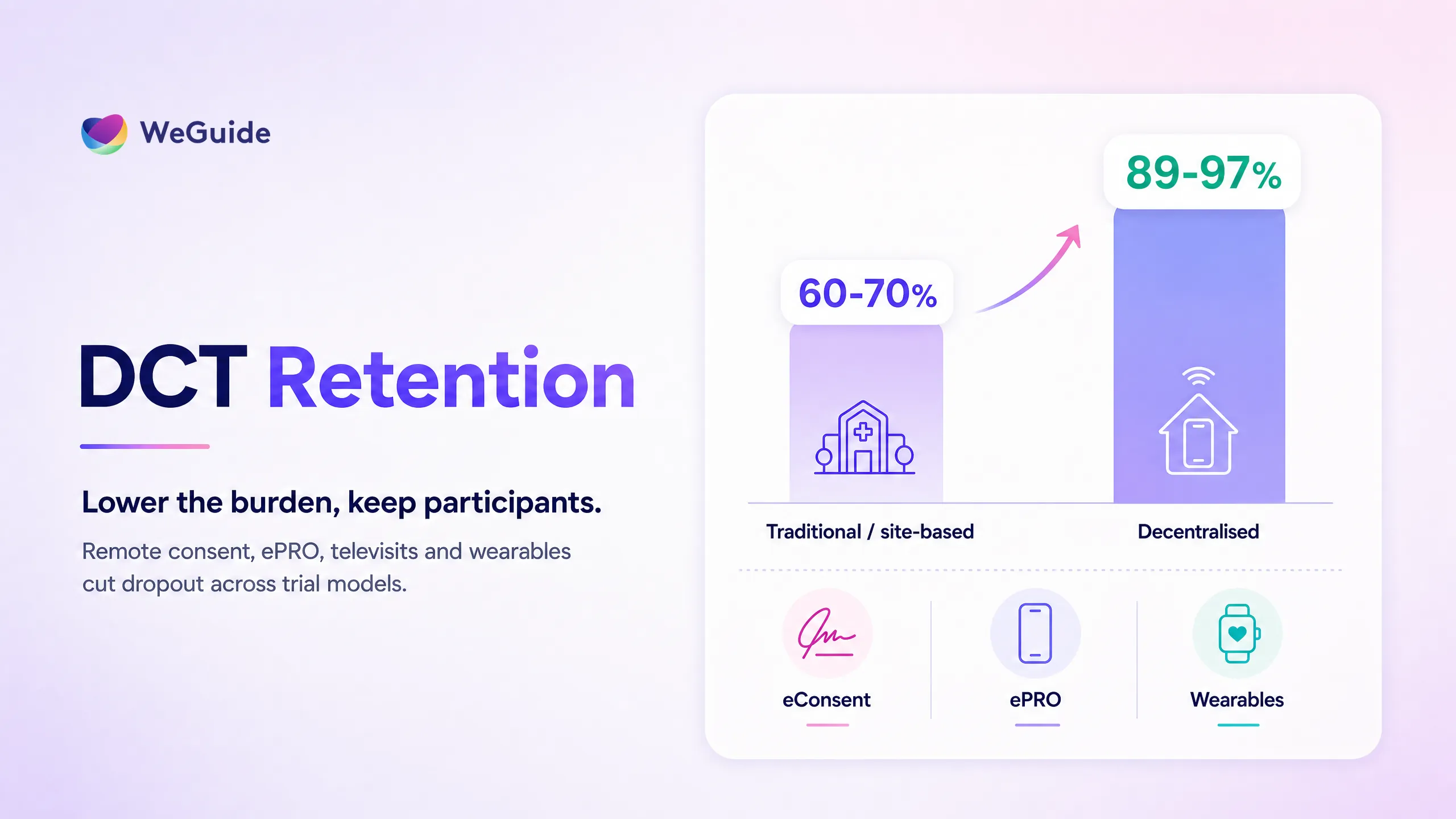

Decentralised clinical trials patient retention improves when remote elements remove the burdens that cause dropout, mainly travel, rigid site visits, and paperwork. By shifting visits, consent, and data capture into participants' homes through televisits, eConsent, ePRO, and wearables, decentralised and hybrid trials have reported retention rates of 89 to 97%, against roughly 60 to 70% in comparable site-based studies.
That gap is the reason clinical operations and patient engagement leads keep asking the same question. Does decentralisation actually move the retention needle, by how much, and through which mechanisms? This article skips the definition and goes straight to the evidence. You'll get a retention-by-model comparison, the burden chain that explains why dropout falls, the honest cases where it doesn't, and a clear steer on what to decentralise first. If you're scoping a remote or hybrid design, our decentralised clinical trial overview pairs well with the operational view below.
Key Takeaways
- Review of 13 studies found 7 reported positive retention, and 4 made direct comparisons favouring decentralised methods.
- 89% vs 60%, up to ~97%. One cited comparison reported 89% retention in the decentralised arm versus 60% in the conventional arm, and a fully decentralised Singapore trial reported about 97% retention.
- Burden removal drives retention. Retention rises because each remote element removes a specific dropout driver: travel, site data entry, paper consent, and clinic vitals.
- Not a universal win. Decentralisation is not a universal win. One large neurodegenerative trial found no statistically significant difference in discontinuation across models.
- Hybrid for complex, fully remote for reach. Hybrid designs often retain best for complex protocols, while fully decentralised designs widen access and diversity.
Do Decentralised Trials Actually Improve Retention?
Yes, in most comparative studies, though not universally. A 2023 systematic review of 13 decentralised clinical studies published in PMC found that 7 of the 13 reported success retaining participants under decentralised methods, and 4 made direct retention comparisons where outcomes favoured the remote approach. In one cited study of lower back pain, the decentralised arm held 89% retention against 60% in the conventional arm.
Newer single-trial data points the same way. The PROMOTE study, a fully decentralised double blind randomised controlled trial run in Singapore and published in Frontiers in Public Health in 2025, reported about 97% participant retention, which the authors put down to the flexibility and low burden of remote participation. These are strong figures against the rough 60 to 70% completion many teams see in site-based studies.
The honest read is directional rather than guaranteed. Retention depends on protocol intensity, population, and how well the remote experience is built. The evidence supports decentralisation as a retention lever, not a magic switch, and the size of the lift varies by trial. For the wider set of causes behind dropout and how to reduce it, see our guide to patient retention in clinical trials.
Retention by Trial Model: Traditional vs Hybrid vs Decentralised
The clearest way to compare models is side by side: typical participant burden, reported retention, diversity impact, and best fit use case. Most published comparisons reference the same handful of trials, so the figures below are cited ranges, not universal benchmarks.
| Trial model | Typical participant burden | Reported retention (cited range) | Diversity and access impact | Best fit use case |
|---|---|---|---|---|
| Traditional / site-based | High: repeated clinic visits, travel, time off work, paper forms | Roughly 60 to 70% completion in comparable studies (per DCT review comparisons) | Limited by geography, narrower reach | Protocols needing frequent on site procedures or specialised equipment |
| Hybrid | Moderate: some on site visits plus remote consent, ePRO, and televisits | High in practice, sits between site-based and fully remote, often retaining best for complex protocols | Broadens reach while keeping clinical touchpoints | Complex or interventional trials that still need periodic site contact |
| Fully decentralised | Low: home based visits, eConsent, wearables, and to-participant logistics | 89 to 97% reported in cited trials (89% lower back pain arm, ~97% PROMOTE) | Widest geographic and socioeconomic reach, 6 of 13 reviewed studies reported diversity gains | Observational, low intervention, or simple interventional designs suited to remote capture |
Read the table as a spectrum, not a ranking. The fully decentralised figures come from trials whose protocols suited remote capture. A complex oncology or device protocol may retain better as a hybrid, because some procedures genuinely need a clinic. The lesson is to match the model to the protocol, not to chase the highest number in someone else's study.
How DCTs Reduce Patient Burden, the Mechanism Behind Retention
Decentralised trials retain participants because each remote element removes a specific burden that drives dropout. Burden is the root cause, and travel sits near the top of it. Industry research from the Center for Information and Study on Clinical Research Participation (CISCRP) consistently finds travel and time among the heaviest participation costs, and a meaningful share of participants travel well over half an hour each way to a site.
Mapping element to burden makes the chain explicit:
- Travel and clinic visits are removed by telehealth visits, so participants attend from home instead of taking time off work.
- Site data entry is replaced by ePRO and BYOD capture, so participants report outcomes from their own phone.
- Paper consent becomes remote eConsent, removing print, post, and a clinic trip just to sign.
- Clinic vitals are captured passively through Garmin and wearable integration, so heart rate, sleep, and activity flow in without effort.
- Language barriers drop away with multilingual support, which keeps non English speakers enrolled.
Remove the burden and you remove the most common reason people leave. For the full burden taxonomy and how to score it across a protocol, our companion piece on reducing patient burden in clinical trials goes deeper than this section can. The short version: retention is a downstream effect of burden, so the highest burden steps are the first ones worth moving off site.
See the DCT layer in action
WeGuide is the patient-facing layer that delivers eConsent, ePRO, telehealth, and wearables for your decentralised or hybrid design, alongside your CTMS and EDC.
Fully Decentralised or Hybrid? Choosing the Right Model for Retention
For complex protocols, hybrid designs often retain best, while fully decentralised designs maximise access and diversity. The right answer depends on protocol intensity rather than a blanket preference for one model.
Hybrid keeps the clinical touchpoints that genuinely need a site, infusions, imaging, or procedures, while shifting everything else remote. That mix can hold participants who would struggle with frequent travel but still need periodic in person care. It also lowers the technology and logistics risk of going fully remote in one step, which matters for first time decentralised teams.
Fully decentralised designs shine when the protocol suits home based capture. They widen geographic and socioeconomic reach, which is where the diversity gains in the 13-study review came from, with 6 of 13 trials reporting more representative samples. The trade-off is that some procedures simply cannot move home, and pushing them remote anyway can hurt data quality. Match decentralisation to the protocol: decentralise what removes burden without compromising the science, and keep in person only what has to be.
Where DCTs Don't Improve Retention, the Honest Caveats
Decentralisation is not a universal retention win. In some trials the difference disappears once you control for population and protocol. A large neurodegenerative trial published in PMC compared discontinuation across models and found 26.28% at traditional sites, 28.17% at decentralised sites, and 28.05% at hub and spoke sites, with no statistically significant difference between them.
Several factors explain when the lift fails to appear. Older or less digitally confident populations may find an app based experience harder, not easier. Device access and connectivity gaps can exclude exactly the participants you hoped to reach. And in conditions where in person assessment is central to the protocol, remote capture adds little.
Tufts CSDD and similar bodies have long noted that under-representation persists even as access tools improve, so decentralisation helps reach but doesn't erase structural gaps on its own.
The practical takeaway is to design for your population. Decentralisation lowers burden for most participants, but the benefit is conditional on tech literacy, device access, and protocol fit. Reporting the null cases honestly is part of building a defensible case, not a reason to avoid the model.
Beyond Retention: Engagement and Diversity Gains
Decentralisation also lifts engagement and widens who can take part. In the 13-study review, 6 of 13 trials reported benefits to sample diversity or population heterogeneity, largely because remote access removes the geographic limits of a fixed site. People who could never reach a city hospital weekly can join from a regional town.
Engagement compounds the effect. When participants interact through an app they already carry, with reminders, education, and progress tracking built in, they stay connected across the clinical trial patient journey rather than only at visits. That continuous contact is the heart of patient engagement software for trials, and it feeds real-time analytics so teams can spot an at risk participant before they go quiet. Engagement and retention move together: the same remote elements that keep people enrolled also keep them active.
A Real Example: The BRACE Trial
The BRACE Trial is a concrete proof point for remote engagement at scale. Run on a custom WeGuide app, it supported more than 6,000 participants across five countries and recorded over 90% participant adherence, with a 6-week deployment during COVID-19 restrictions. Participation ran through mobile data capture, wearables, and remote workflows rather than routine clinic visits.
What makes BRACE useful here is the honesty of the claim. It's one trial, in a specific design, not proof that every decentralised study reaches the same number. But it shows that high adherence across borders is achievable when the remote experience is built around the participant, with reminders, education, and low friction reporting doing the retention work. You can read the BRACE Trial case study for the full picture, and the published 12-month outcomes sit alongside it as the clinical record.
What to Decentralise First
Start with the highest burden steps that don't compromise the science. Consent, patient-reported outcomes, and routine check ins are usually the easiest wins, because moving them remote removes travel and paperwork without touching the clinical core of the protocol.
A practical order of operations:
- Move consent to eConsent so participants enrol without a site trip.
- Shift outcome reporting to ePRO and passive wearable capture.
- Add televisits for check ins that do not require physical procedures.
- Keep only the procedures that genuinely need a clinic in person.
WeGuide is the patient-facing layer that delivers this remote experience: eConsent, ePRO and eCOA, education, reminders, multilingual, wearables, telehealth, and analytics in one branded app. It supports your decentralised design rather than replacing your CTMS or EDC. For broader context on engagement across the trial lifecycle, the pillar guide on patient engagement in clinical trials ties these elements together, and our guide to patient centricity in clinical trials shows the operating model behind this approach in practice.
Frequently Asked Questions
Do decentralised clinical trials improve patient retention?
In most comparative studies, yes. A systematic review of 13 decentralised studies found 7 reported positive retention, and one cited comparison showed 89% retention in the decentralised arm versus 60% conventional. The lift is directional and depends on protocol and population, not guaranteed in every trial.
How do decentralised trials reduce patient burden?
Each remote element removes a specific cost of participating. Televisits remove travel, ePRO and BYOD capture remove site data entry, eConsent removes paper and a signing trip, and wearables capture vitals passively. Since burden is the leading driver of dropout, removing it directly supports retention.
What is the dropout rate in decentralised vs traditional trials?
It varies by trial. Cited decentralised trials report retention of 89 to 97%, against roughly 60 to 70% completion in comparable site-based studies. Some trials show no significant difference, so the gap reflects protocol fit and population rather than a fixed dropout rate per model.
Are hybrid clinical trials better for retention than fully decentralised?
Often, for complex protocols. Hybrid designs keep the in person procedures that genuinely need a site while shifting consent, reporting, and check ins remote, which suits interventional studies. Fully decentralised designs maximise access and diversity and fit simpler or observational protocols best. Match the model to protocol intensity.
Do decentralised trials improve diversity and access?
They help. In the 13-study review, 6 of 13 trials reported benefits to sample diversity or population heterogeneity, mainly because remote access removes geographic limits. Decentralisation widens reach but doesn't erase structural under-representation, which still needs deliberate recruitment and inclusive design to address.
What technology drives engagement in decentralised trials?
The core stack is eConsent for remote enrolment, ePRO and eCOA for outcome reporting, wearables for passive data, telehealth for remote visits, multilingual support for access, and analytics for monitoring. Delivered through one branded app with reminders and education, these tools keep participants active between touchpoints. Our guide to clinical trial patient engagement software compares how these platforms work in practice.
Conclusion
The evidence supports a clear, qualified answer. Decentralised and hybrid trials improve patient retention in most comparative studies, with cited figures of 89 to 97% against roughly 60 to 70% site-based, because each remote element removes a specific burden that drives dropout. The honest caveat matters too: some trials show no difference, so the benefit depends on protocol fit, population, and how well the remote experience is built.
Map your protocol to the right model
Walk through how WeGuide's patient-facing layer removes the burdens that drive dropout across your decentralised or hybrid design.
Book a demoNo pressure, just a conversation.

