
.svg)
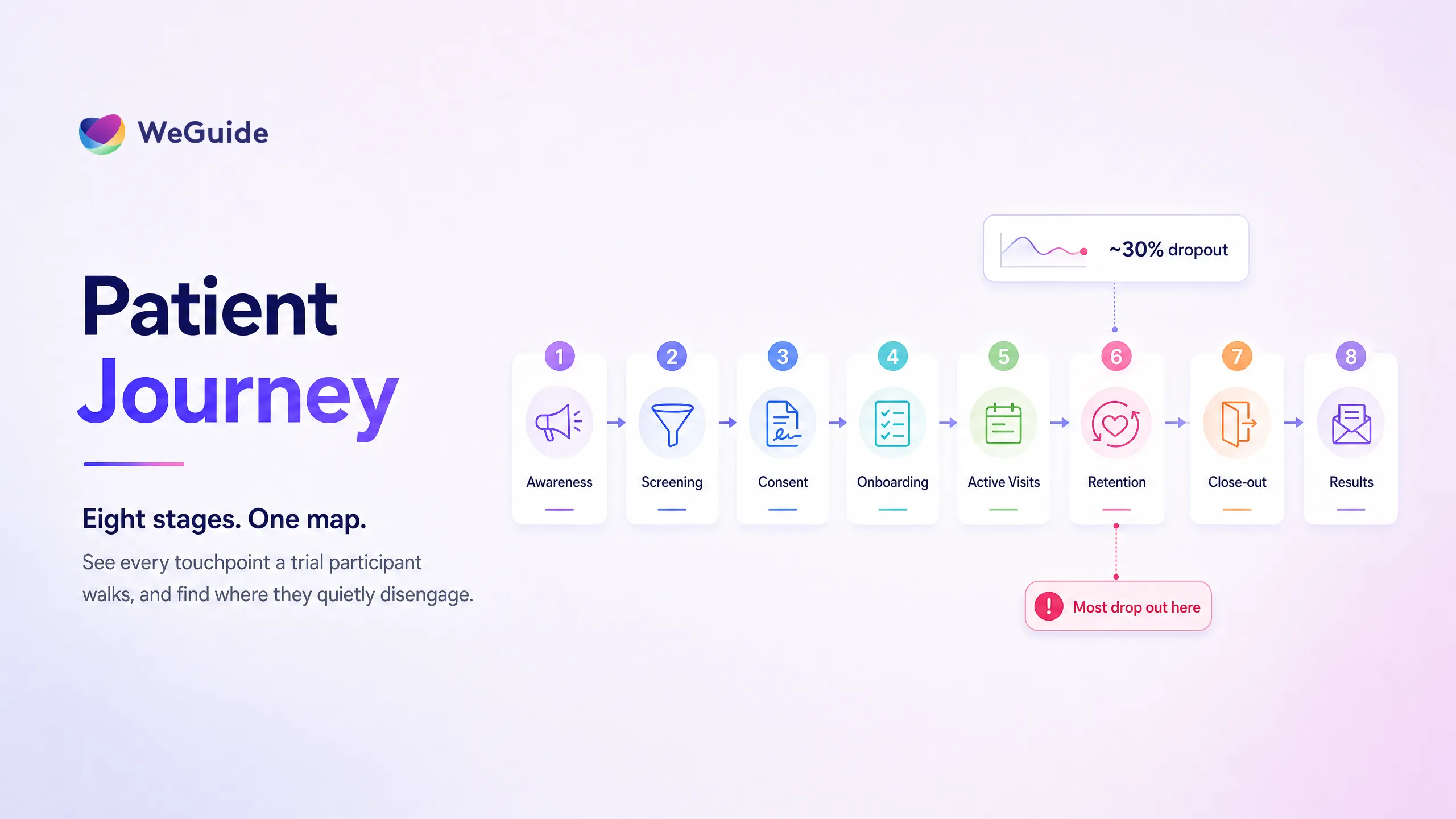

The clinical trial patient journey is the full path a participant travels, from first becoming aware of a study, through screening, informed consent, and onboarding, to active visits, data capture, retention, close out, and results sharing. Each stage carries a distinct risk of disengagement, and most dropout traces back to participant burden that builds across these touchpoints.
Most maps of this journey stop at consent or active visits. That's a problem, because the stages teams forget are exactly where participants quietly fall away. Up to 1 in 4 enrolled participants don't finish the trial they join, and the 2020 Onsite analysis puts average dropout near 30% in some datasets, within a wider range of roughly 15% to 40% depending on the trial.
This guide maps all eight stages on one screen, names the engagement risk at each, and points to the digital lever that reduces it. If your job is to find the friction that drives screen fails and attrition, our patient engagement software operates across most of these touchpoints, and this article shows you where.
Key Takeaways
- Eight journey stages. The clinical trial patient journey runs across eight stages: awareness, pre screening, informed consent, onboarding, active visits and data capture, retention, close out, and results sharing.
- Disengagement peaks mid-trial. Most participants disengage during the long active and retention stretch, where cumulative burden, travel, and poor communication add up rather than any single side effect.
- Dropout is rising. One Applied Clinical Trials analysis found average dropout rose from 15.3% to 19.1% over seven years, a roughly 25% increase.
- Journey is not experience. Patient journey is the sequence of stages. Patient experience is how each stage feels to the participant.
- Every stage has a lever. Each stage has a clear digital lever, from plain language eConsent to remote data capture and returning lay results.
The 8 Stages of the Clinical Trial Patient Journey at a Glance
The clinical trial patient journey runs across eight stages, and each one carries its own engagement risk and its own lever to reduce it. Mapping the journey this way turns a vague concept into a usable tool. You can point to a single stage, name what's pulling participants away, and assign the fix that holds them.
The table below puts the whole journey on one screen. Read it top to bottom as the path a participant actually walks, then use the rest of this article to go deeper on whichever stage matters most for your study.
| Stage | What happens | Where participants disengage (the risk) | The engagement lever | WeGuide capability |
|---|---|---|---|---|
| 1. Awareness and discovery | A person first hears a relevant trial exists | Trust and relevance gap, the source doesn't feel credible | Clear, plain language information from a trusted channel | Patient facing education and multi language reach |
| 2. Pre screening and eligibility | First check against the criteria | Friction and screen fail frustration | Fast digital screening that pre qualifies | Screening module |
| 3. Informed consent | The participant decides to join | Confusion and low health literacy lead to withdrawal | Plain language, multimedia eConsent with comprehension checks | eConsent |
| 4. Onboarding and education | Expectations are set | Mismatch between expected and actual demands | In app education that sets realistic expectations | Patient education module |
| 5. Active visits and data capture | The longest, highest burden stretch | Visit and diary fatigue, missed entries | Remote ePRO, reminders, and bring your own device | Form Builder and DCT support |
| 6. Retention | Staying engaged over time | Cumulative burden, travel, lost to follow up | An engagement layer: reminders, telehealth, data back to patient | Telehealth and reminders |
| 7. Close out | The participant exits the study | Abrupt exit and post trial uncertainty | Structured off boarding and completion analytics | Analytics dashboard |
| 8. Results sharing | Lay results return to participants | Participants feel used and won't re enrol | Returning plain language results | Patient engagement layer |
Stage 1: Awareness and Discovery
Awareness is where a person first learns a relevant trial exists, and it sets the tone for the entire clinical trial patient journey. People hear about trials in more than 20 different ways, but the PMC systematic review found they consistently prefer to hear it from their own physician. A message from a trusted clinician carries weight that an advert rarely matches.
The risk here is a trust and relevance gap. If the information feels generic or the source feels unfamiliar, interest dies before screening starts. The lever is clear, plain language information delivered through a channel the person already trusts. Reaching people in their own language matters too, which is where multi language support and patient education widen the top of the funnel.
This article doesn't cover recruitment tactics. For sourcing, channel mix, and outreach, read our guide to clinical trial recruitment strategies. At scale, engagement infrastructure has reached large populations. The WeGuide built GenV study supports more than 100,000 families, which shows what a well designed awareness and enrolment layer can hold.
Stage 2: Pre Screening and Eligibility
Pre screening is the first real touchpoint, the moment a person checks whether they fit the criteria. It's also the first place the journey leaks. The risk is friction and screen fail frustration. Long forms, repeated questions, and slow responses push interested people away before anyone has spoken to them.
The lever is fast digital screening that pre qualifies people quickly and respectfully. A short, mobile friendly questionnaire can filter out clear non matches and route eligible people straight to a site, so staff spend their time on real candidates. WeGuide's screening module handles this first filter digitally, which cuts the wait that turns early interest into a no.
Screen failure will always happen, and that's healthy. The goal isn't to qualify everyone. It's to make the check quick and clear so the people who don't fit aren't left frustrated and the people who do fit don't drop out of impatience.
Stage 3: Informed Consent
Informed consent is the make or break moment of the journey, because it's where comprehension either holds or breaks. The participant has to understand what they're agreeing to, including the time, the procedures, and the risks. When consent documents are dense and written above the reader's health literacy, confusion follows, and confusion drives early withdrawal.
The risk is low comprehension. The lever is plain language, multimedia eConsent with comprehension checks built in. Short videos, simple summaries, and quick knowledge checks help participants genuinely understand the study rather than skim and sign. WeGuide's eConsent module presents consent in plain language with multimedia and comprehension prompts, which supports better understanding at the point of decision.
Regulatory note: Always consult your IRB or ethics committee before implementing eConsent. Requirements vary by jurisdiction, and the right adviser will confirm what your study needs.
Better consent isn't only an ethical duty. A participant who truly understands the commitment is far less likely to leave when the demands of the study become real.
Stage 4: Onboarding and Education
Onboarding is where expectations get set, and it's the quiet gap between saying yes and showing up. The participant has consented, but they may not yet grasp the rhythm of visits, the diaries, or the devices ahead. The risk is a mismatch between what they expected and what the study actually asks of them.
The lever is in app patient education that sets realistic expectations early. When people know what's coming, how often, and why each step matters, they're far more prepared to stay the course. WeGuide's patient education module delivers this guidance inside the same app participants already use, so onboarding feels like support rather than paperwork.
Good onboarding also reduces avoidable questions for site staff. A participant who understands the schedule from day one needs fewer reminders and makes fewer mistakes, which protects both data quality and the relationship.
Engagement across every stage
WeGuide's participant-facing engagement layer operates across these touchpoints, sitting alongside your CTMS and EDC rather than replacing them.
Stage 5: Active Visits and Data Capture
Active participation is the longest and highest burden stretch of the clinical trial patient journey, and it's where fatigue sets in. This is the phase of repeated visits, electronic patient reported outcome (ePRO) diaries, and ongoing data capture. The risk is visit and diary fatigue, with missed ePRO entries and skipped visits adding up over weeks and months.
The lever is remote data capture that fits around the participant's life. Mobile ePRO with reminders, bring your own device entry, and remote visits reduce the load without losing data quality. WeGuide's Form Builder captures ePRO and eCOA on the participant's own phone, and a decentralised clinical trial design moves more of the burden off site entirely. For how remote models change engagement and dropout in particular, see our guide to participant engagement and retention in decentralised trials. The tooling that runs this stage is covered in our breakdown of clinical trial patient engagement software.
This is where a strong engagement layer proves itself. In the BRACE trial, a BCG vaccine study, the WeGuide platform supported more than 6,000 participants and held high adherence through a long and demanding follow up, as documented in the BRACE trial case study. Reducing per visit friction is what carries people through the hardest stretch.
Stage 6: Retention, Where Most Participants Disengage
Retention is the stage where most participants actually disengage, and it rarely comes down to a single dramatic reason. Drug side effects are not the top driver of dropout. The real causes are cumulative: travel, time away from work, poor communication, and a slow drip of burden that finally outweighs the participant's motivation. Lost to follow up is the quiet end state of all of it.
The risk is this build up of burden over time, and lowering it is its own discipline, covered in our guide to reducing patient burden in clinical trials. The lever is an engagement layer that keeps the relationship warm. Timely reminders, telehealth visits that remove travel, and giving participants their own data back all raise perceived value and lower the cost of staying in. The 2020 Onsite analysis and Applied Clinical Trials both point to logistics, communication gaps, and financial strain as the drivers, not medical events.
Retention deserves its own playbook, and this hub deliberately doesn't list tactics here. For the full strategy, read the pillar on patient engagement in clinical trials and the dedicated guide to patient retention in clinical trials.
Stage 7: Close Out
Close out is the stage where a participant formally exits the study, and a clumsy exit leaves a sour final impression. After months of regular contact, an abrupt end can feel like being dropped. The risk is post trial uncertainty: participants unsure what happens next, whether they keep their study treatment, or who to contact.
The lever is structured off boarding paired with completion analytics. A clear final visit, plain instructions on what comes next, and a thank you all close the relationship well. On the operational side, WeGuide's analytics dashboard shows completion patterns across the cohort, so teams can see who finished, who didn't, and where in the journey the leaks occurred.
A clean close out protects more than goodwill. Participants who leave a study feeling respected are the ones most likely to recommend research to others and to join again.
Stage 8: Results Sharing and Post Trial
Results sharing is the stage almost everyone forgets, and it's the one that decides whether a participant ever comes back. Once data is locked, lay results are too often never returned. The risk is that participants feel used, like a data point rather than a partner, and that feeling makes them far less likely to re enrol or to encourage others.
The lever is simple: return plain language results to the people who made the study possible. A short, accessible summary of what the trial found closes the loop with respect. Doing this well sits squarely within the patient engagement software layer, which keeps a channel open to participants after the active study ends.
Results sharing is where patient centricity becomes real rather than a slogan. It costs little and it builds the trust the whole research enterprise depends on for the next study.
Patient Journey vs Patient Experience: What's the Difference?
The patient journey is the sequence of stages a participant moves through. The patient experience is how each of those stages feels to them. The journey is the map. The experience is the weather along the route.
Both matter, and they shape each other. A well designed journey with smooth touchpoints produces a good experience, while hidden friction at any single stage can sour the experience even when the overall path looks fine on paper. Designing the journey around the participant, rather than around site convenience, is what patient centricity in clinical trials means in practice. A real example of that design in action is a patient centric app for a decentralised trial, built to keep the experience light while the journey ran its full course.
How to Explain a Clinical Trial to a Patient
Explaining a clinical trial to a patient works best when you walk them through the journey in plain language, stage by stage. Keep it concrete and honest about what each step asks of them.
You might say it like this. First, you'll learn about the study and check whether you fit. If you do, we'll explain everything in detail and answer your questions before you decide anything. If you choose to join, we'll show you what to expect, then you'll attend visits and answer some questions over time, some of which you can do from home.
We'll stay in touch and support you throughout, and when the study ends, we'll tell you what we found. The point is to set realistic expectations and make clear that the participant is a partner, not a test subject.
Frequently Asked Questions
What are the stages of a clinical trial patient journey?
The clinical trial patient journey has eight stages: awareness and discovery, pre screening and eligibility, informed consent, onboarding and education, active visits and data capture, retention, close out, and results sharing. Each stage is a touchpoint where a participant can either stay engaged or quietly drop away from the study.
Where do patients most often drop out of clinical trials?
Most participants disengage during the long active and retention stages. The cause is rarely a single side effect. It's cumulative burden: travel, time away from work, poor communication, and financial strain that build up over months, according to analyses from 2020 Onsite and Applied Clinical Trials, until they outweigh the participant's motivation to continue.
What is patient journey mapping in clinical trials?
Patient journey mapping is the practice of laying out every stage and touchpoint a participant moves through, from awareness to results sharing, so a team can see where friction and disengagement risk concentrate. It turns a vague idea of the participant experience into a shared, usable map for finding and fixing dropout.
How long does the clinical trial patient journey take?
It varies widely by study, from a few weeks to several years. The awareness, screening, and consent stages can take days to weeks, while the active and retention stages span the trial's duration, often many months. Close out and results sharing extend the journey well past a participant's final study visit.
What's the difference between the patient journey and patient experience?
The patient journey is the ordered sequence of stages a participant travels through. The patient experience is how each of those stages actually feels to them. The journey is the structural map of touchpoints, while the experience is the emotional and practical reality of moving along that path.
Bringing the Journey Together
Mapped end to end, the clinical trial patient journey makes one thing clear: dropout isn't a single event but a series of small disengagements across eight stages. The teams that retain participants are the ones that name the risk at each touchpoint and put a lever against it.
- Map all eight stages, not just consent and active visits.
- Treat retention and results sharing as design problems, not afterthoughts.
- Reduce per stage burden with screening, eConsent, education, remote data capture, and telehealth.
- Return lay results so participants stay partners for the next study.
See the engagement layer in action
Walk through how WeGuide supports participants across every stage of the journey, alongside your existing trial systems.
Book a demoNo pressure, just a conversation.

